Codeine and Morphine Pathway, Pharmacokinetics
Summary
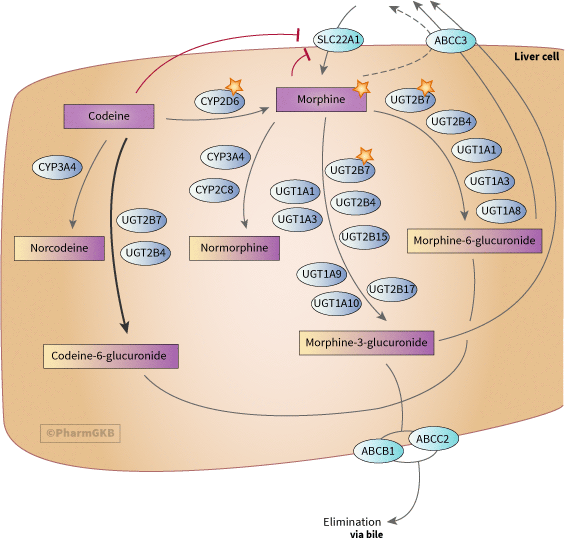
Representation of the candidate genes involved in metabolism of codeine and morphine.
Description
This pathway depicts, in a stylized human liver cell, the principal candidate pharmacogenes involved in the pharmacokinetics of codeine and morphine. Modulation of the pharmacokinetic conversion of codeine to morphine by variation in the CYP2D6 gene is a well-known example of pharmacogenetics. Below is a brief summary of the main gene and drug relationships [Article:17339873][Article:18597654]. This pathway was originally published in 2009 [Article:19512957], the online version has been updated to include new candidate genes and clinical PGx guidelines and recommendations.
Background
Codeine and morphine are pain relief drugs in the opioid family. Both drugs are found naturally in the poppy plant, Papaver somniferum, but for commercial use, codeine is usually synthesized from morphine, which is more abundant in nature. In addition to their analgesic effects, both drugs have antitussive effects and antidiarrheal activity. Side effects include respiratory depression, constipation, sedation, tolerance, nausea, vomiting, itch, dry mouth and addiction. Codeine is a less potent agonist of the mu opioid receptor (MOR, coded for by the OPRM1 gene) than morphine and is considered a safer alternative in an outpatient setting. However, over the past thirteen years [Article:16920476][Article:18719619][Article:30467830][Article:30545525] there have been reports of particular patient groups at risk for major adverse events which have led to labeling changes for codeine, these are discussed below in the clinical guideline section.
Metabolism
The principal pathways for metabolism of codeine occur in the liver, although some metabolism occurs in the intestine and brain [Article:18187562][Article:8875123]. Approximately 50–70% of codeine is converted to codeine-6-glucuronide by UGT2B7 [Article:9010622]. Approximately 10–15% of codeine is N-demethylated to norcodeine by CYP3A4. Norcodeine and codeine-6-glucuronide both have a similar affinity to codeine for the MOR [Article:8818573]. Between 0 and 15% of codeine is O-demethylated to morphine, the most active metabolite, which has 200-fold greater affinity for the MOR compared with codeine. This metabolic reaction is performed by CYP2D6 [Article:2049245][Article:1867957][Article:18781855].
Approximately 60% of morphine is glucuronidated to morphine-3-glucuronide, M3G, while 5–10% is glucuronidated to morphine-6-glucuronide, M6G [Article:8841154][Article:18187562]. N-demethylation to normophine is considered a minor pathway and catalyzed mostly by CYP3A4 with some contribution from CYP2C8 [Article:12936704]. M6G is considered to be highly active, with greater analgesic activity than morphine while M3G does not appear to play a role in pain relief but may influence other actions or side effects [Article:16796385] Formation of M6G and M3G in the liver is principally catalyzed by UGT2B7, while UGT1A1 may have a minor role in the formation of M3G [Article:12185559]. UGT1A1 and UGT1A8 are capable of catalyzing the formation of M6G in vitro and so contribute to this pathway, although UGT1A8 is minimally expressed in liver [Article:18187562]. Other studies with recombinant proteins showed the capability of UGT2B4 in both M3G and M6G generation [Article:12920168][Article:18187562]. Generation of M3G was much higher for UGT2B7 but small amounts were generated by UGT1A1, UGT1A3, UGT1A9, UGT1A10, UGT2B4, UGT2B15 and UGT2B17 [Article:12920168][Article:18187562]. For M6G, UGT2B7 was the greatest generator, with minor roles for UGT2B4, UGT1A8, UGT1A1 and UGT1A3 [Article:12920168]. UGT2B4 was equal to UGT2B7 in production of codeine-6-glucuronide [Article:12920168].
Pharmacogenomics
The most well studied gene with respect to the pharmacogenetics of this pathway is CYP2D6 (80% of variant annotations on codeine involve CYP2D6). The CYP2D6 gene is highly polymorphic with many important single nucleotide polymorphisms, haplotypes and copy number variants (see CYP2D6 VIP annotation for further details)[Article:19512959]. Simplistically, CYP2D6 variants can be categorized into poor metabolizers, PMs, (low or zero activity variants), normal metabolizers NMs (high or normal activity variants, also called extensive metabolizers), intermediate metabolizers IMs and ultrarapid metabolizers UMs (multiple gene copy variants)[Article:19512959]. An individual's highest functioning CYP2D6 allele predicts his/her phenotypic activity [Article:16968950][Article:14618296] (e.g. NM allele and PM allele results in an NM phenotype, UM allele and NM allele results in UM phenotype, IM allele and PM allele results in IM phenotype, etc.). NMs possess at least one fully functional CYP2D6 allele, and are thought of as phenotypically normal. CYP2D6 PMs are unable to convert codeine to morphine efficiently and as a consequence may not experience pain relief, although this may differ between experimental pain paradigms and clinical pain [Article:17339873][Article:1782973]. UMs may metabolize codeine too efficiently leading to morphine intoxication [Article:9357099][Article:15625333].
One paper reported a CYP2D7 genetic variant resulting in a frame shift that activated the pseudogene creating a protein that is able to metabolize codeine to morphine, this was not confirmed by later studies [Article:15051713][Article:30040020].
Although not as extensively studied in this context as CYP2D6, other pharmacogenes have been shown to influence this pathway. Variation in CYP3A4, or coadministration of drugs that act at CYP3A4, can affect flux through the codeine pathway with sometimes fatal consequences [Article:15625333][Article:24747667]. The FDA label cautions about cotreatment of codeine with either CYP3A4 inhibitors or CYP3A4 inducers and suggests “careful consideration of the effects on the parent drug, codeine, and the active metabolite , morphine” (see annotated drug label at https://www.pharmgkb.org/chemical/PA449088/label/PA166104916).
There is conflicting evidence regarding the influence of UGT2B7 polymorphism on codeine and morphine metabolism. The most well studied single nucleotide polymorphism, UGT2B7*2 (rs7439366, UGT2B7:His268Tyr, UGT2B7:802T>C) did not effect morphine metabolism in vitro [Article:12920168][Article:11186130]. Additional variants in UGT2B7 have been shown to impact morphine metabolism in some studies but have failed to be consistently reproduced [Article:12811366][Article:17724700][Article:18622261]. With the recent identification of the haplotype structure of UGT2B7 and identification of variants affecting mRNA splicing, future studies will be able to better define the role of variation in this gene on the codeine and morphine pathway [Article:18622261].
Transporters are also depicted in this pathway, as they influence clearance of codeine, morphine and their metabolites [Article:12492606][Article:15886284]. Some of the evidence for the involvement of these transporters was derived from experiments done in mice and may or may not be translatable to human pharmacokinetics [Article:12950465][Article:10516633]. The transporters present at the blood–brain barrier, not depicted in this pathway, as well as metabolic enzymes and transporters in the brain and gastrointestinal tract, also play an important role in the pharmacokinetics of codeine and morphine. There is growing evidence that variants in ABCB1 may influence morphine efflux from the blood–brain barrier and result in variable drug response, with a small study showing a slight effect of ABCB1 variants, another study showed that ABCB1:3435C>T and the receptor variant OPRM1:118A>G had a significant effect on analgesia in cancer patients treated with morphine [Article:16580900][Article:17898703]. Low activity variants in SLC22A1 have been associated with increased likelihood of side effects in healthy individuals treated with codeine, and with increased plasma morphine compared with high activity variants [Article:23835420]. Functionally important variants in other transporters ABCC2, ABCC3 and SLCO1B1 have been documented and may also be important for the pharmacokinetics of codeine and morphine, although this has yet to be demonstrated [Article:15530129].
Clinical Guidelines
In 2007 the FDA added a warning to the codeine drug label to caution use of codeine in breastfeeding mothers due to reports of infant deaths (FDA page no longer available). In 2013, the label was changed to add a contraindication stating that codeine should not be used in children after tonsillectomy or adenoidectomy because of risk for respiratory depression and death (pdf of archived FDA release). In 2017 this was broadened to contraindicate codeine and tramadol (another opioid metabolized by CYP2D6, see pathway) in all children under 12 [Article:28520700]. FDA cites their own investigation “Reviewing adverse event reports submitted to FDA from 1969 to 2015 identified 64 cases of serious breathing problems, including 24 deaths, with codeine-containing medicines and from 1969 to 2016 nine cases of serious breathing problems, including three deaths, with use of tramadol in children younger than 18. Most serious side effects with both codeine and tramadol occurred in children younger than 12 years, and some cases occurred after a single dose.” Similar restrictions in Europe and Canada were also issued in 2013 [Article:27647717]. In 2015 the Ethiopian Food Medicine and Health Care Administration and Control Authority placed a temporary ban on use of codeine, citing studies that have shown an incidence of UM of around 30% https://allafrica.com/stories/201511241318.html.
CPIC guidelines for codeine and CYP2D6 first issued in 2011 and updated in 2014 [Article:22205192][Article:22205192]. The guideline gives recommendations for dosing changes or alternative medications in patients for whom genotyping data on CYP2D6 variants and copy numbers is available: for individuals who are CYP2D6 NMs, the evidence is strong that codeine is safe and can be dosed at standard levels, for PMs or UMs there is strong evidence for avoiding codeine use, there is moderate evidence that standard doses of codeine are safe for IMs, although if no pain relief is observed, an alternative medication should be chosen.
The American Academy for Pediatrics supports the overall ban of codeine use in children, but suggests more data is needed on PGx in pediatric populations and additional data on the safety of alternative analgesics in pediatric populations [Article:27647717]. Since the relative abundance of drug metabolizing enzymes in the liver changes during child development for both the CYP and UGT families of enzymes, this needs consideration when assessing PGx impact [Article:19476420][Article:29737521]. For example, neonatal levels of UGT1A4, 1A6, 1A9, and 2B7 are more than 10-fold lower than adults and children don’t reach 50% protein abundance of adult livers until 2-10 years depending on isoform thus potentially influencing intrinsic clearance for morphine [Article:29737521]. Preliminary data in pediatric patients with sickle cell disease showed that PGx prescribing allowed for continued safe use of codeine in children who were not CYP2D6 UM or PMs [Article:27335380]. Consideration should be given to PGx guided codeine use in children where they are unlikely to experience adverse effects and alternatives are not safer/of unknown safety or as effective [Article:30467830].
Improved training in PGx in the clinical setting is also needed. Reports show that codeine still being used in pediatric cases and that there is a lack of understanding from both physicians and pharmacists as to why and when codeine is inappropriate [Article:30181719].
Authors
Citation
Please consult the citation policy on how to cite this pathway.
Therapeutic Categories
- Pain, anti-inflammatory and immunomodulating agents